‘Rigor and Research in Healthcare Design: A Decade of Advocacy’: Which level are you in Evidence-Based Practice?

Kirk Hamilton

Kirk Hamilton
The McMorrow Reports is excited to bring you bi-monthly excerpts from the industry-acclaimed Evidence-Based Design resource book Rigor and Research in Healthcare Design: A Decade of Advocacy.
The book was written by Kirk Hamilton, FAIA, FACHA. Hamilton is a Professor of Architecture, Texas A&M University, a Founding Principal of WHR Architects and a board member of The Center for Health Design. He is also an editor of Health Environments Research & Design Journal. Hamilton has published more than 30 articles, many of which are featured in the book, on Evidence-Based Design (EBD) in HERD and Healthcare Design magazine.
Herman Miller Healthcare, working in collaboration with Hamilton and Vendome Group compiled many of the architect’s writings into this single, printed publication.
“Kirk has been one of the industry’s leading voices on the process and the value of evidence based design in healthcare and we’re honored to have the opportunity to bring a decade worth of his work on the subject together in this comprehensive single volume,” said Phyllis Goetz, EDAC, PVDN, Director, Healthcare Strategic Programs and Services for Herman Miller.
In the coming weeks, The McMorrow Reports for Healthcare Facilities Management will be taking a closer look at chapters on The Four Levels of Evidence-Based Practice; Evidence, Decisions, Guidelines and Standards; Ten Suggestions for Increasing Rigor in Architecture & Design; and Flexibility, Differential Obsolescence, and Measurement.
Excerpted from Chapter 2: The Four Levels of Evidence-Based Practice
Evidence-Based: Meaning and Scope Evidence-based healthcare designs are used to create environments that are therapeutic, supportive of family involvement, efficient for staff performance, and restorative for workers under stress. An evidence-based designer, together with an informed client, makes design decisions based on the best information available from research and project evaluations. Critical thinking is required to develop an appropriate solution to the design problem; the pool of information will rarely offer a precise fit with a client’s unique situation. In the last analysis, though, an evidence-based healthcare design should result in demonstrated improvements in the organization’s clinical outcomes, economic performance, productivity, customer satisfaction, and cultural measures.
Researchers in the area of the physical environment and healthcare have been reporting their results for some time. Roger Ulrich, PhD (1984), conducted a pioneering study disclosing that surgery patients with a view of nature suffered fewer complications, used less pain medication, and were discharged sooner than those with a view of a brick wall.
Research by others shows that heart patients with strong social support systems survive longer post-discharge than those without. There are studies on the antimicrobial characteristics of new carpet fibers, appropriate lighting for neonates, the negative effects of noise on critical care patients, and many more on a wide range of subjects that impact the design of health facilities (for a sampling, see References and Suggested Reading). In all, approximately 120 credible evidence-based design studies had been identified by 2003 as having specific environmental relevance.
Authors currently preparing a book on critical care design are using more than 300 research citations from multiple literature sources. By 2008, Ulrich and colleagues had identified more than 1,200 citations from the scientific literature relating the environment to clinical outcomes. …
Evidence-Based Practice: Four Levels
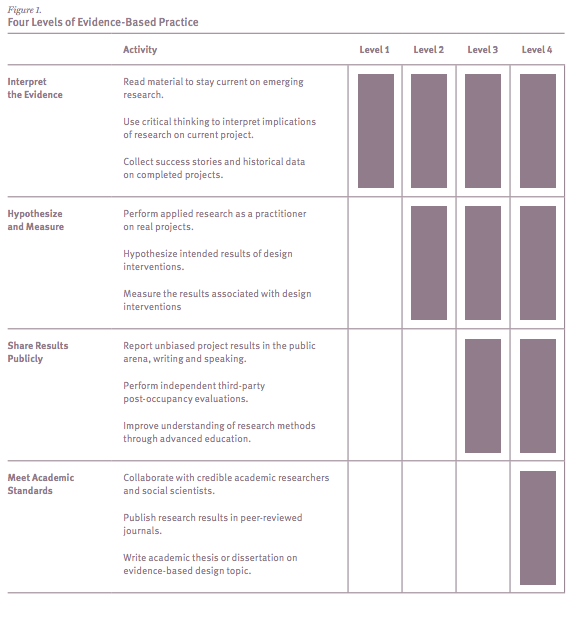
Four “levels” can be used as a means to identify different commitments and practices as stages in which architects use this material on behalf of their clients (Figure 1 – to the right).
What are the four levels of Evidence-Based Practice? Click the image to enlarge.
To explain: Level-one practitioners: These architects and design professionals make a careful effort to design based on the available evidence. They make an effort to stay current with literature in the field. The designer interprets the meaning of the evidence as it relates to his or her project, and makes a judgment as to the best design for that specific circumstance.
These designers are producing work that advances the state of the art because they are learning from others and developing new examples for others, while delivering better designs for their clients. …
Level-two practitioners: Evidence-based practitioners at level two take another important step. Based on readings, they hypothesize the expected outcomes of design interventions and subsequently measure the results. This level of attention makes design less subjective and requires attention to new ways to design. At this level, the designer must understand the research, interpret its implications, and be able to build a chain of logic to connect the design decision to a measurable outcome. This discipline reduces the number of arbitrary design decisions in healthcare projects and delivers solutions linked to outcomes. It also raises the challenge of preventing bias from reducing objectivity in the gathering and reporting of results. The evidence-based practitioner must strive for the truth and resist the temptation to tilt the reporting of findings to emphasize success or downplay failure….
Level-three practitioners: In addition to following the literature, hypothesizing the intended outcome of their design interventions, and measuring the results, these designers report their results in the public arena. Publishing in the popular press or speaking at conferences makes an important contribution to the field and advances the state of the art. It also subjects the designers’ methods and results to the scrutiny of others who may or may not agree with them. These practitioners soon learn they need to better understand research methods and often seek some level of advanced education to promote greater rigor in their documentation of results. …
Level-four practitioners: Practitioners/ scholars at this level perform the same tasks as those at the other levels—following the literature, hypothesizing the outcomes of design interventions, measuring the results, and reporting in the public arena. These practitioners take the next step by publishing in quality journals that require review by qualified peers. They may also collaborate with social scientists in academic settings who contribute to the formal literature. These level-four evidence-based practitioners are working directly in the field, designing and building operating healthcare facilities, but they are also subjecting their work to the highest levels of rigorous review and formally advancing the useful evidence in the field. …
In my experience, the best way to filter the nearly overwhelming pool of information sources is to use an orderly design process. Establishing the project goals at the outset helps the team identify the significant design issues and problems to be addressed. Opportunities for evidence-based design can be identified in the programming and pre-design phase. The available research is then combed for material relevant to the narrower list of those design issues. Judgment is then required to sort potentially conflicting implications of the research.
Rigor and Research in Healthcare Design: A Decade of Advocacy is available for healthcare leaders, architecture and design professionals, as well as college students enrolled in healthcare design programs only through Herman Miller. You can request a copy of the book by contacting Anne Parks via email: anne_parks@hermanmiller.com
You also can pick up a copy Nov. 15 to 18 at the Healthcare Design Conference in San Diego. The book will be featured in the Herman Miller Healthcare/Nemschoff booth (No. 1001 ) in the exhibit hall.